

The role of Micro-Hospitals in Healthcare Expansion
Micro-hospitals are small inpatient care facilities that are more easily financed and deployed than larger, traditional hospital programs. They offer a specific solution to address patient care gaps within a healthcare system by improving access for patients requiring lower acuity care. Without planning foresight, micro-hospitals are nothing more than buildings within a healthcare system that will run their course in providing any real value and stand in the way of program change and growth. Micro-hospitals should be seen as the first step in providing growth and flexibility, not a final step in expanding a healthcare system’s reach.
The Micro-hospital Model
Programmatically, micro-hospital facilities have a minimum of four inpatient beds, although operationally eight to ten beds are recommended. Additional programs typically include lab, imaging, surgery, pharmacy, and emergency departments. Total building size lands between 20,000 and 70,000 square feet. Often these facilities are planned and constructed in underserved areas, ranging from urban to rural, as a means of expanding a healthcare system’s geographic footprint. Requirements for function and compliance are the same for all hospitals regardless of size. Micro-hospitals are still held to the same Conditions of Participation for Medicare reimbursement and are certified as short-term acute care hospitals. They must also be “primarily engaged” in the provision of inpatient services and comply with the Emergency Medical Treatment and Active Labor Act (EMTALA) to ensure public access to emergency services regardless of ability to pay. Because micro-hospitals focus on lower acuity care, there is dependence upon arrangements with larger hospitals for transport and care of patients with higher acuity needs.
Operational Challenges: Balancing Staffing Needs
Micro-hospitals can be agile and reduce overhead costs through employing caregivers with flexible skillsets, and optimally managed staff to patient ratios. The objective is to address less acute cases, reduce length of stay, and deliver the care that is needed at a less costly location. The operational challenge to healthcare systems is properly balancing this management, as there are ideal metrics that align staffing with the smaller size of micro-hospitals. Emerus, a national leader in emergency, inpatient and diagnostic healthcare, successfully pioneered this, but without this alignment the smaller size and program of a micro-hospital may not be viable for a healthcare system. For this reason, healthcare systems often look to complement the minimum program requirements of a micro-hospital with other service lines where billing is more profitable.
Future-Proofing Healthcare Facilities
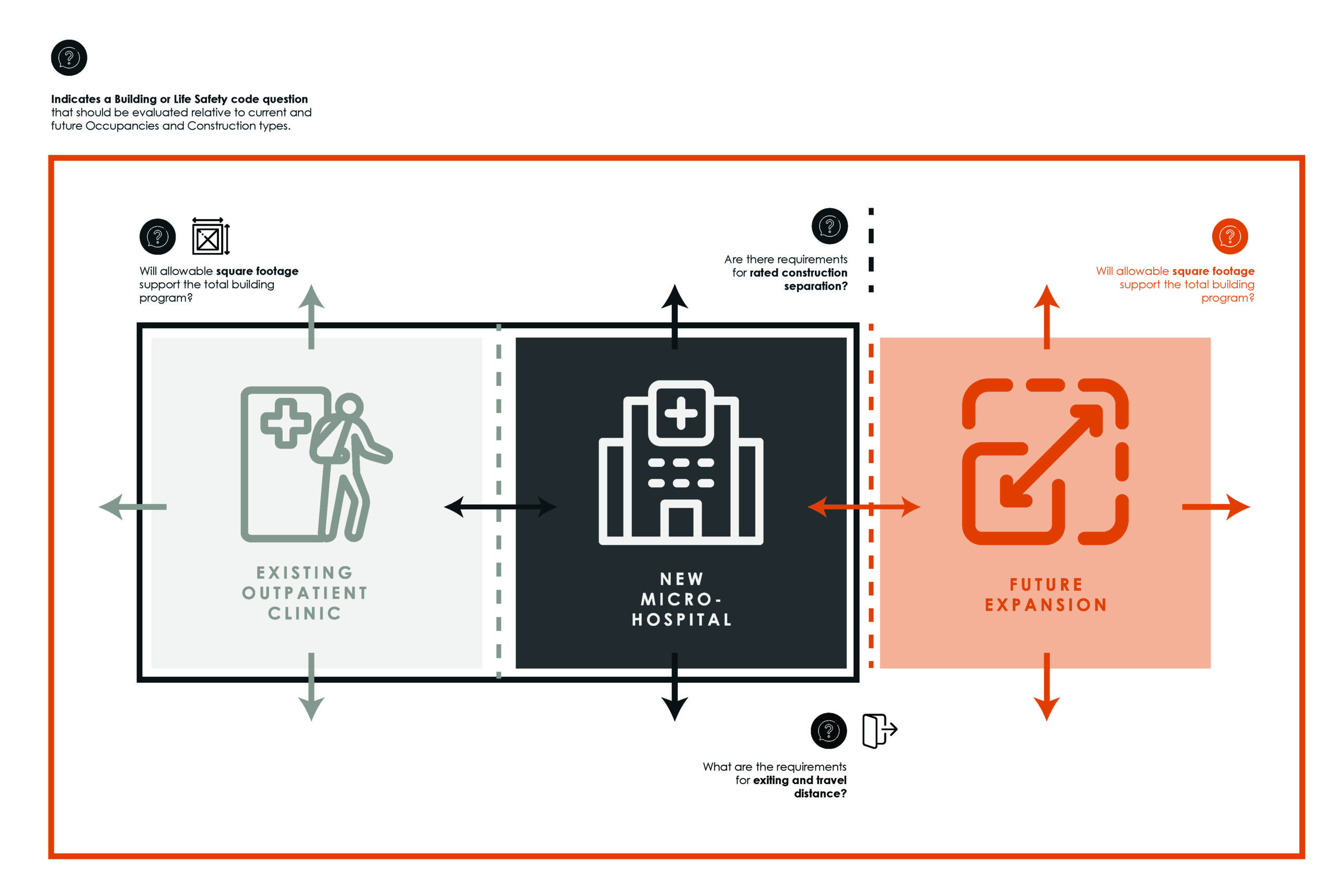
Data Bridge Market Research estimates the micro-hospital market to have been $250 billion in 2022, with 8% annual growth projected to take this to $460 billion by 2030. The financial numbers support the idea that micro-hospitals are solidly part of the current healthcare landscape. The question is how these projections look further out. Hospital facilities are typically constructed to serve healthcare systems for 50 to 100 years. An 8-year outlook is just a fraction of this. The greatest challenge to micro-hospitals is also one that is unseen. It is the limitation to long-term utility due to building codes that are applied today without consideration for the growth and flexibility that will be required tomorrow. Healthcare systems run the risk of committing to lower capital investments that do not future-proof buildings. Codes consider how buildings are occupied and used, type of construction that will be required, size limitations, and how these may need to be separated from other buildings on site (spatially or through specific construction requirements). If there are not code considerations that account for the long-term goals of a healthcare system, there may be no added future utility for the micro-hospitals we are building today.
Micro-hospitals’ Strategic Evolution
Micro-hospitals are valuable in their ability to meet current, specific challenges that healthcare systems are facing; but this typology runs the risk of being irrelevant before these buildings reach their full life expectancy. Programmatically they offer limited and focused care, operationalizing and staffing can be challenging to balance, and there is still dependence on larger healthcare systems for more acute care needs. In addition, lack of foresight in planning and construction may negate the future flexibility that is valued in all healthcare projects. The isolated micro-hospital projects that have peppered barren healthcare markets are at an end. Instead, these facilities will evolve, through renovation and expansion, or turn back into a newer version of a mid-size community or neighborhood hospital – but only if today’s planning sets up for this future state. Without the appropriate application of building codes and thoughtful planning, micro-hospitals stand as a real estate and financial risk to healthcare systems. To remain viable and sustainable assets, micro-hospitals can no longer be thought of as stand-alone facilities, but as the first step in growth and flexibility.